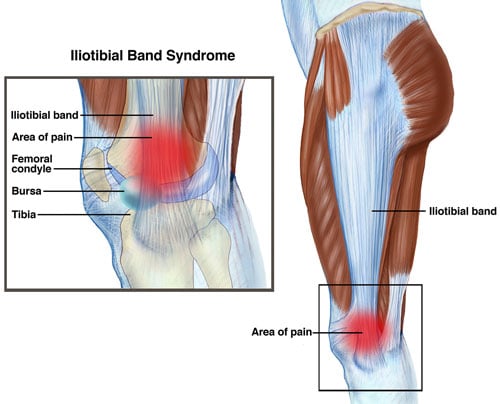
 ITB = Ilio-Tibial Band. The ITB is a muscle that runs from the ilium to the tibia. The ilium is the boney wing of your pelvis. The tibia is the big leg bone between your knee and ankle. The ITB has a short little contractile muscle belly on the side of your hip, and a long, non-contractile tendon down the side of your thigh, that anchors onto the bone on the outside of the knee. And that’s where it gets sore in runners. ITB soreness is called “runner’s knee”.
Tendons are the weak link when we overtrain or start new exercise programs. The muscle belly has a good blood supply. We draw them as red on anatomy posters, and the tendon we draw as white, representing the fact that it doesn’t have as much blood. When we train, the muscle belly copes well with whatever we throw at it, but the tendon can let us down. All the overtraining injuries we get are sore tendons: Achilles, ITB, Tennis Elbow, sore Rotator Cuffs, etc. Tendons don’t like the combination of load and stretch. Achilles get sore when we run up hill, putting the tendon on a stretch. Tennis elbows get sore when we hit backhands “late”, which combines stretch and load to the tendon. ITBs don’t like the stretch/load combination in runners who let their knees turn in. Ultimately, doing too much too quickly is the cause. Because it would never be sore if you never ran. But the biomechanics of your gait are a contributor. It’s more common in women than men, because women have wider pelvises, their thigh bones start wider apart at the top, and angle in more than men’s (called a Q-angle). We test a single leg squat and see where your knee points, in relation to your foot, and that predicts where your knee travels when you run. Ideally we like the knee to move over the foot. In runners who get runner’s knee, we often see your knee travels more to the inside of the foot. We call this femero-tibial internal rotation. People commonly call it "knock knees”. Biomechanical contributors to this can be:
Letting the knee twist in, or the hips move out laterally, puts the ITB on more of a stretch. The ITB protests by getting sore. There’s usually a spike in training load that sets it off. One long run, or more runs per week than usual. If you increase gradually, it adapts. The initial pain is inflammatory, although it doesn’t always look swollen. If you can rest it for a couple of weeks, and treat it with ice and anti-inflammatory tablets, it usually settles down well. If you run on it when it’s already sore, it can turn into a more chronic problem that takes ages to heal. I get people to not run for 2 weeks, while you do a couple of strength/control exercises:
On the second week I get you to increase your walking distance. Once you can go for a decent walk without the knee being sore, I’ve got a jogging program that builds you up from 1min through to a 5km, over three or 4 weeks. We add in harder strength exercises as you go. Comments are closed.
|
�
Archives
July 2024
Categories
All
|
 RSS Feed
RSS Feed
|
|


|
MENU
|
INJURY INFO
|
INJURY INFO
PHYSIO MOSMAN |
Copyright© 2024| Fit As A Physio | ABN 62855169241 | All rights reserved | Sitemap